
Anthrax (Bacillus Anthracis) – N, N1
Perhaps Anthrax is mostly known as the “powder letter” agent due to Amerithrax cases in 2001, when citizens started eating Ciproxin like sweets. However, Anthrax is a common natural agent that can be found almost all around the word…
Anthrax Biological Agent Description
Anthrax is a serious infectious but not contagious disease caused by Bacillus anthracis bacteria. Anthrax can be found naturally in soil and wild animals around the world. Anthrax can cause severe illness in both humans and animals. People can get sick if they come in contact with infected animals or contaminated animal products, eat food or drink water contaminated with spores or breathe in spores and get spores in to the body. Spores can also enter the human body through a cut or scrape of the skin. Once inside, anthrax spores become active and multiply producing toxins which cause the illness.
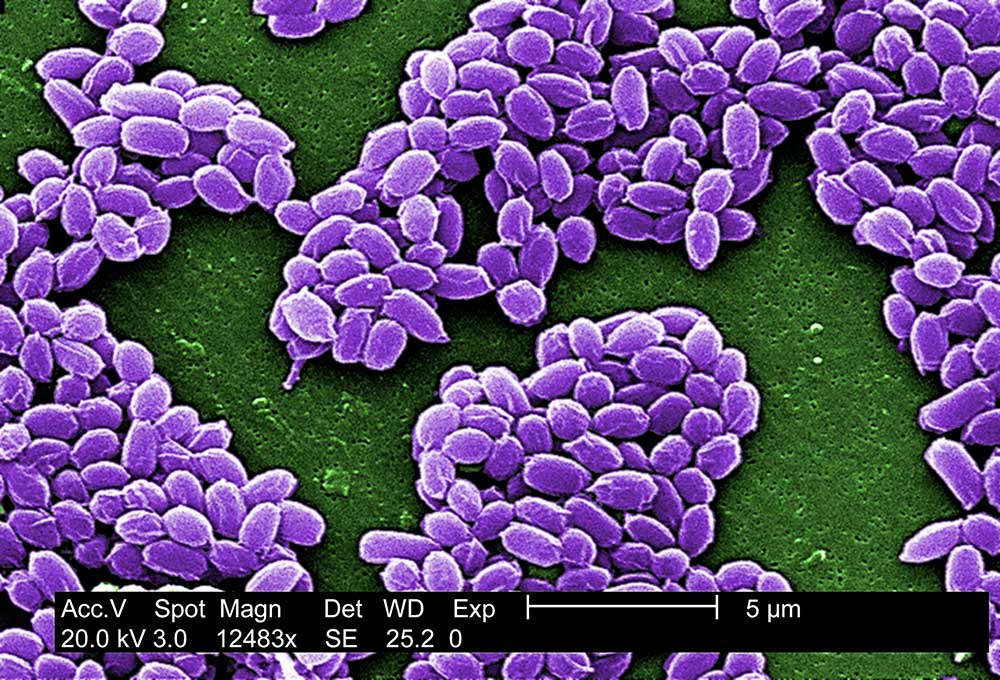
Bacillus anthracis dormant spores (not active), that can live in natural environment.
When anthrax spores get inside the body, they can be “activated.” When they become “active”, the bacteria can multiply, spread, produce toxins (poisons), and cause severe illness. This can happen when people breathe in spores, eat food or drink water that is contaminated with spores, or get spores in a cut or scrape in the skin.
Anthrax is most common in agricultural regions of Central and South America, sub-Saharan Africa, central and southwestern Asia, southern and eastern Europe, and the Caribbean. Even if anthrax is rare in other areas, sporadic outbreaks can occur in wild and domestic grazing animals such as cattle or deer.
Anthrax is one of the most likely biological agents to be used in an intentional release — biological attack or bioterrorism with anthrax — to sicken or kill people, livestock or crops. The microscopic spores could be put into powders, sprays, food, and water. Anthrax spores are not able to be seen, smelled, or tasted. Anthrax became a major concern following Amerithrax in 2001, when there were several incidents that impacted both public health and safety, when several buildings became contaminated and people died from exposures to anthrax spores.
Anthrax Historical Background
Anthrax is thought to have originated in Egypt and Mesopotamia in ancient times, dating back to 700 BC. Ancient Greece and Romans have written registers regarding deaths and illnesses caused by anthrax.
The first clinical descriptions of cutaneous (“skin”) anthrax were given by Maret in 1752 and Nicolas Founier in 1768 from malignant pustules. French Philibert Chabert first published of anthrax as a specific disease from dead animals in 1780. During the 1800s, doctors saw anthrax cases and links, but did not yet have a diagnosis for it because the organism that caused anthrax wasn’t discovered yet.
Scientist Robert Koch discovered in 1877 that anthrax bacteria formed spores, and that these were able to survive for long periods and in many different environments. He developed and used his famous Koch Pustulates. A few years later in 1881 Louis Pasteur created the first vaccine for anthrax.
Max Sterne created the anthrax vaccine for animals in 1937, which reduced anthrax cases in humans. Even though the penicillin had been discovered in 1928, it was only used for the first time to treat anthrax in 1944. It took until the 50s for the first anthrax vaccine for human to be created and it had 92.5% effectivess in preventing cutaneous (“skin”) anthrax. This vaccine was used for two decades, until the same vaccine that is still used today was released in the 1970s.
In early 2010 a new form of anthrax was discovered from a small outbreak in United Kingdom and Germany among heroin drug users. This form was called injection anthrax and the anthrax spores were believed to be present in the heroin.
Anthrax Usage
Robert Koch discoveries boosted more sophisticated experiments and created knowledge on how to produce large stocks of germs. There is evidence that the German army secretly infected livestock and animal feed traded to the Allied Nations by neutral partners. For instance, related to this Argentinian livestock infection in 1917 and 1918 resulted the death of 200 mules.
The Geneva Protocol for the Prevention of the Use in War of Asphyxiating, Poisonous or other Gases and Bacteriological Methods of Warfare was created in 1925. This treaty was a great step in trying to stop the use of biologic agents during war.
Japanese Army’s Unit 731 under Surgeo Lieutenant General Shiro Ishii produced and conducted biological weapons research in Japanese occupied Manchuria in 1932. Japan not only tested anthrax by giving it into prisoners, but also attacked at least against 11 cities spraying anthrax and other biological agents from aircrafts.
The United Kingdom and United Nations had a biological weapons program conducted experience with anthrax in 1942. Weapons were tested in Mississippi and Utah. They prepared to respond against German if needed with 5000 anthrax bombs. The United Kingdom had live agent anthrax widespread test in Guinard Island off Scotland coast. The island was uninhabitable until 1986 because long staying anthrax spores.
During the Korean war the US biological weapons program was expanded. The program also included vaccines development and biological agent protection. By 1960s US possessed a large collection of biological weapons.
The United Kingdom submitted a proposal to the United Nations in July 1968 to prohibit the development, production, and stockpiling biological weapons. In the same year, the Warshal Pact also submitted a similar proposal. In the next year, the US terminated their biological weapons program and adopted the policy to never use any biological weapons or toxins under any circumstances. After these actions, the research was directed to defence and protection methods.
In 1972 the Convention on the Prohibition of the Development, Production, and Stockpiling of Biological and Toxin Weapons and on Their Destruction was signed and ratified in April of the same year.
There was a deadly anthrax outbreak in Sverdlovsk, USSR, from April to May of 1979. This outbreak came in light in western countries not until early 1980. This consisted of an accidental airborne anthrax spore leak in Soviet military microbiology facility, causing 96 human casualties 4 kilometres downwind from the facility. The Soviet Union maintained the natural outbreak-legend until 1992, when Boris Yeltsin admitted the true.
In Autumn 2001, two US Senators’ offices and news media agencies along the East Coast got anthrax spore filled mail. Four letters with post marked 18th September to 9th October 2001 were identified. The powder from the letters contaminated buildings and people. The first case of anthrax was diagnosed on 4th October. During the next two months a total of 11 confirmed cases of inhalation (7 postal workers) and 11 cutaneous anthrax were registered. One of the infected was a 94-year-old who was infected via cross-contamination in a mail facility. From 22 infected persons, 5 died. In all, 43 people tested positive for anthrax exposure and more than 10 000 people were considered at risk of possible anthrax exposure. After a 7-year FBI investigation, the anthrax spore origin was found from a specific research laboratory and Dr. Bruce Ivins a single actor in planning and executing these attacks. This Amerithrax case is estimated to have costed the US a total of 1 billion US dollars.
Anthrax Transmission & Dispersion
Anthrax has low infectiousness and does not transmit from person-to-person. Inhaled anthrax is the most serious form and can kill quickly if not treated immediately. This type of attack would mean the anthrax spores could easily be blown around by the wind or carried on people’s clothes, shoes, and other objects. It only takes a small amount of anthrax to infect a large number of people. In military use, there have been delivery methods for anthrax like missiles, bomblets, artillery, and also point and line airborne release methods.
Anthrax Exposure Symptomology
Anthrax infections types effect on symptoms and incubation times from 1 day to 2 months. The inhalation infection dose is approximately 2000 – 50 000 spores.
- Inhalation (pulmonary) anthrax symptoms are: fever and chills, chest discomfort, shortness of breath, confusion or dizziness, cough, nausea, vomiting, or stomach pain, headache, sweats (often drenching), extreme tiredness and body aches. The incubation time is typically 1-7 days but can also be up to 60 days.
- Cutaneous (“skin”) anthrax symptoms are: small blisters or bumps that may itch, swelling around the sore, a painless skin sore with a black center on the face, neck, arms or hands after the small blisters or bumps witch most often the sore. The incubation time is typically 1 day.
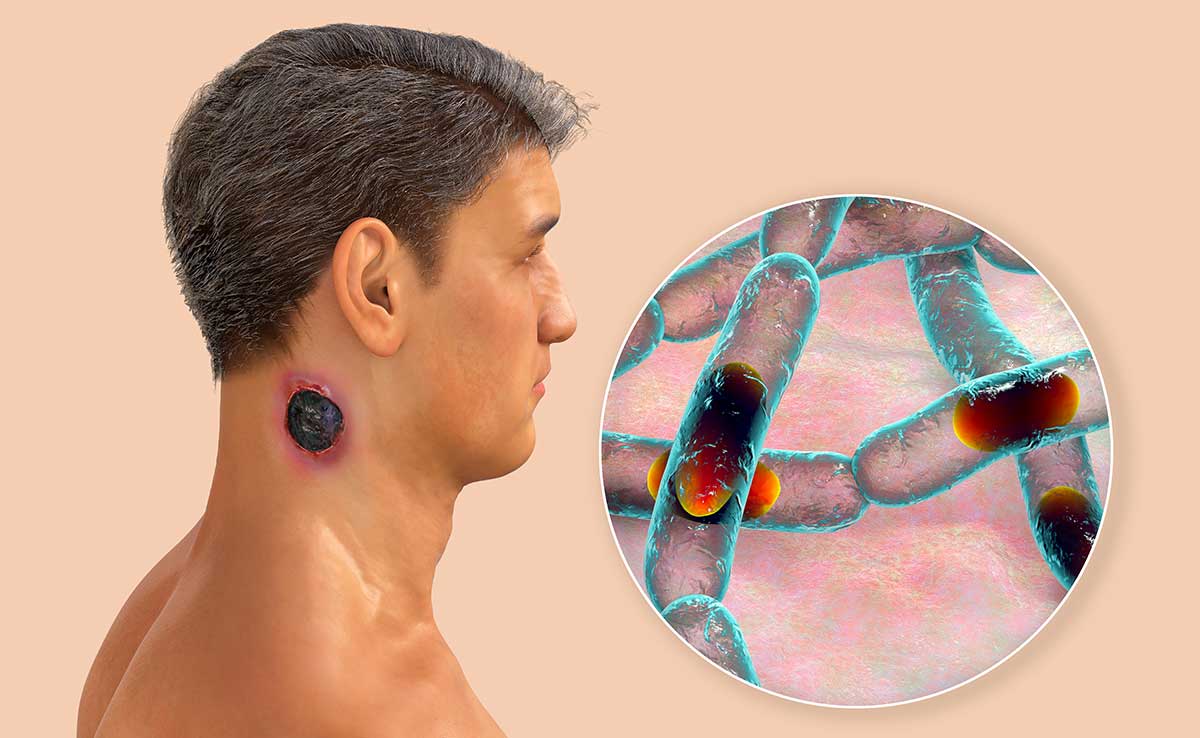
Cutaneous anthrax, the most common form of anthrax infection, manifested by a characteristic black eschar on the neck skin, and closeup view of bacteria Bacillus anthracis.
- Gastrointestinal anthrax symptoms are: fever and chills, swelling of neck or neck glands, sore throat, painful swallowing, hoarseness, nausea and vomiting (especially bloody vomiting), diarrhea or bloody diarrhea, headache, red face and red eyes, stomach pain, fainting, swelling of stomach. The incubation time is typically 3-7 days.
- Injection anthrax symptoms are similar to those of cutaneous anthrax, but injection anthrax can spread throughout the body faster and be harder to recognize and treat than cutaneous anthrax.
Anthrax Infection Treatments
All types of anthrax infection can be treated with antibiotics (example of penicillin, ciprofloxacin, doxycycline). Anthrax antitoxins are also available to use when the anthrax spores activate in the body and start to produce toxins. The vaccination in humans is not common without any critical reason.
Untreated cutaneous anthrax case-fatality rate is 5 – 25 %, inhalation and gastrointestinal nearly 100 % on delayed or without treatment.
Response & Protection Actions Against Anthrax
Operators should use the highest protection level if the situation is unknown, with potential biological agents disseminating via air, the concentration is possibly high, and there are also other vapour or splash hazards. The protection level can decrease if the aerosol-generator is not on anymore, or if the biological agents and hazard level is defined or the “letter” or “package” can be easily bagged.
For infectious substances, the hazardous area is where the substance is dispersed. The isolation distance for dust / powder / liquid is 25 meters for all directions and for downwind 100 meters. Isolate the room and even the building if the event is takes place indoors. Do not shake or empty the content of suspected package, and do not carry it anywhere.
Decontaminate the protection clothing and equipment after the use, and before cleaning, or disposal with a compatible chemical disinfectant (like 10% bleach solution or 0,5% sodium hypochlorite or through decontamination systems (like autoclave).
Did You Know?
There have been two anthrax cases in 2006 and 2009 where people were diagnosed with anthrax that came from animal skin drums. The anthrax spores contaminated the skin in a natural way.
Anthrax has also a UN 2814 number for infectious substances affecting humans.
Anthrax Fact Box
| Agent type | Bacteria |
| Infectiousness | Low |
| Person-to-Person | No |
| Incubation period | 1-6 days |
| Infectious dose (aerosol) | 2000 – 50000 spores |
| ENVI Assay Sensitivity | 105 spores/ml sample buffer |
| Lethality | Untreated 25% (cutaneous), nearly 100% (pulmonary/gastrointestinal) |
| Therapy | Vaccine, antibiotics |
ENVI Assay System
Bertin Environics’ ENVI Assay System bio defence tests is the ideal tool for provisional identification of Biological threats. These high quality and proven tests for early detection are the most compact immunoassay “lab-in-a-box” in the market.
Disposable, separate assays for seven highly poisonous hazardous agents: ricin toxin, botulinum toxin, Bacillus anthracis anthrax, orthopox virus, SEB, Yersinia pestis and Francisella tularensis.
Leave a Reply